Tags
abortion, Democratic Party, Planned Parenthood, reproductive rights, Roe v. Wade, U.S. election 2024, Vice President Kamala Harris

Vice President Harris addresses the media after touring a Planned Parenthood women’s health clinic to give support to abortion providers.
____________________________________________________________________
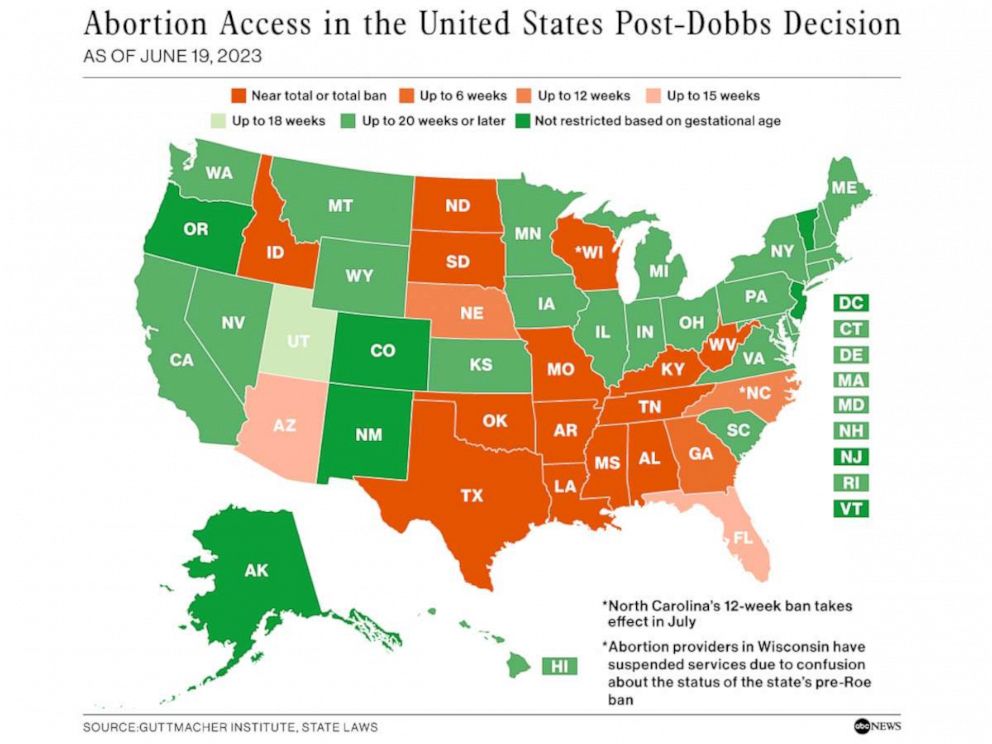
The overturning of Roe v. Wade has resulted in insanities such as the Alabama Supreme Court’s recent declaration that the embryos used by fertility clinics are “children” and must be treated as such. And the anti-abortion measures of Texas, Idaho, and other misogynist states have led to difficult conditions not only for women seeking abortions but also for women experiencing pregnancy complications. There is, however, an intriguing bright spot amid all the doom and gloom.
Since June 2022 Democratic politicians have been making reproductive rights a key part of their platforms. Prior to the reversal of Roe v. Wade most Democratic politicians, if pressed, would voice support for abortion legality. But the support was often tepid at best, and politicians would be uncomfortable about being identified too closely with the issue. President Biden’s 2020 campaign, for example, barely mentioned abortion rights. In part Biden’s reticence and that of other Democrats was because most Democratic strategists believed voters saw abortion rights as only one of a range of important issues. Polls indicated that swing voters, even though most supported reproductive rights, were unlikely to vote for a Democrat primarily for that reason.
Now, the situation is quite different. As The New York Times political correspondent Lisa Lerer noted, “When the Supreme Court overturned Roe v. Wade in June 2022, it created shock waves that reverberated through American politics, helping Democrats stave off a Republican rout in the midterm elections.” The repercussions are still being felt. A late February poll conducted by KFF, a nonprofit organization focused on health policy, indicated that the overturning of Roe v. Wade energized many voters and made them unwilling to shrug off a politician’s dismissal or downplaying of the abortion issue. About 12% of the voters surveyed said that abortion would be the “most important issue” for them this November. That included 28% of Black women, 22% of Democrats, 19% of women in states where abortion is banned and 17% of women aged 18 to 49. Of the voters who said that abortion was the most important issue for them, fully two-thirds said it should be legal in all or most situations.
This is a large change from polls conducted before Roe v. Wade was overturned, in which it was abortion opponents who were most likely to describe themselves as single-issue voters. Now, even among Republican voters, about 40% think abortion should be legal in all or most circumstances, and 43% support drafting federal legislation to secure abortion rights. In other words, even some Republican politicians are going to need to tread carefully to avoid antagonizing constituents alarmed by the consequences of the overturn of Roe v. Wade.
Meanwhile, Democratic politicians are making reproductive rights a cornerstone of their 2024 campaign strategy. On March 14 Vice President Kamala Harris visited a Minneapolis women’s health center and talked with abortion providers there. She was accompanied by Minnesota governor Tim Walz, who in 2023 signed legislation protecting abortion rights and abortion providers in the state. (Minnesota abortion providers have experienced a 36% rise in the number of women seeking abortions due to the restrictive anti-abortion laws of neighboring states.)
This visit by Vice President Harris is believed to be the first time a U.S. president or vice president has toured an abortion clinic. The visit is part of the current White House initiative (led by the Vice President) to highlight the importance of abortion rights and the centrality of the issue in the November 2024 elections.
Sources: Lisa Lerer, “A New Generation of Abortion Voters,” The New York Times, March 11, 2024; Lisa Lerer and Nicholas Nehamas, “Kamala Harris Will Visit Abortion Clinic, in Historic First,” The New York Times, March 14, 2024.