Bromo Selzer douches, pregnancy protection amulets, pennyroyal teas, birch bark tampons, slippery elm sticks — these are but a few of the myriad methods women in different parts of the world have used in their efforts to prevent unwanted pregnancy. Meanwhile, the obstacles they have had to confront have included religious proscriptions, punitive law codes, persecution of midwives, and the devaluing of folk knowledge.
Sex and Herbs and Birth Control is a lively, provocative account of women’s attempts to provide themselves with as wide a range of reproductive options as possible. A more detailed description of the book and ordering information can be found here.
The overturning of Roe v. Wade has resulted in insanities such as the Alabama Supreme Court’s recent declaration that the embryos used by fertility clinics are “children” and must be treated as such. And the anti-abortion measures of Texas, Idaho, and other misogynist states have led to difficult conditions not only for women seeking abortions but also for women experiencing pregnancy complications. There is, however, an intriguing bright spot amid all the doom and gloom.
Since June 2022 Democratic politicians have been making reproductive rights a key part of their platforms. Prior to the reversal of Roe v. Wade most Democratic politicians, if pressed, would voice support for abortion legality. But the support was often tepid at best, and politicians would be uncomfortable about being identified too closely with the issue. President Biden’s 2020 campaign, for example, barely mentioned abortion rights. In part Biden’s reticence and that of other Democrats was because most Democratic strategists believed voters saw abortion rights as only one of a range of important issues. Polls indicated that swing voters, even though most supported reproductive rights, were unlikely to vote for a Democrat primarily for that reason.
Now, the situation is quite different. As The New York Times political correspondent Lisa Lerer noted, “When the Supreme Court overturned Roe v. Wade in June 2022, it created shock waves that reverberated through American politics, helping Democrats stave off a Republican rout in the midterm elections.” The repercussions are still being felt. A late February poll conducted by KFF, a nonprofit organization focused on health policy, indicated that the overturning of Roe v. Wade energized many voters and made them unwilling to shrug off a politician’s dismissal or downplaying of the abortion issue. About 12% of the voters surveyed said that abortion would be the “most important issue” for them this November. That included 28% of Black women, 22% of Democrats, 19% of women in states where abortion is banned and 17% of women aged 18 to 49. Of the voters who said that abortion was the most important issue for them, fully two-thirds said it should be legal in all or most situations.
This is a large change from polls conducted before Roe v. Wade was overturned, in which it was abortion opponents who were most likely to describe themselves as single-issue voters. Now, even among Republican voters, about 40% think abortion should be legal in all or most circumstances, and 43% support drafting federal legislation to secure abortion rights. In other words, even some Republican politicians are going to need to tread carefully to avoid antagonizing constituents alarmed by the consequences of the overturn of Roe v. Wade.
Meanwhile, Democratic politicians are making reproductive rights a cornerstone of their 2024 campaign strategy. On March 14 Vice President Kamala Harris visited a Minneapolis women’s health center and talked with abortion providers there. She was accompanied by Minnesota governor Tim Walz, who in 2023 signed legislation protecting abortion rights and abortion providers in the state. (Minnesota abortion providers have experienced a 36% rise in the number of women seeking abortions due to the restrictive anti-abortion laws of neighboring states.)
This visit by Vice President Harris is believed to be the first time a U.S. president or vice president has toured an abortion clinic. The visit is part of the current White House initiative (led by the Vice President) to highlight the importance of abortion rights and the centrality of the issue in the November 2024 elections.
Sources: Lisa Lerer, “A New Generation of Abortion Voters,” The New York Times, March 11, 2024; Lisa Lerer and Nicholas Nehamas, “Kamala Harris Will Visit Abortion Clinic, in Historic First,” The New York Times, March 14, 2024.
In previous blog posts, I’ve noted the sweeping consequences for women’s reproductive health of the draconian bans on abortion that went into effect after the U.S. Supreme Court overturned Roe v. Wade. Obviously, women in the “red” states must flee to the blue states to get abortions or furtively attempt to obtain abortion pills that are illegal in their state from out-of-state internet sources. But also, as many commentators have stressed, the reverberations of the anti-woman policies in large portions of the U.S. have spread far beyond their intended targets. Any woman who is pregnant or intending to become pregnant, or indeed, any woman seeking timely and competent gynecological care, can be put in danger as a consequence of the fanaticism of the anti-abortion zealots.
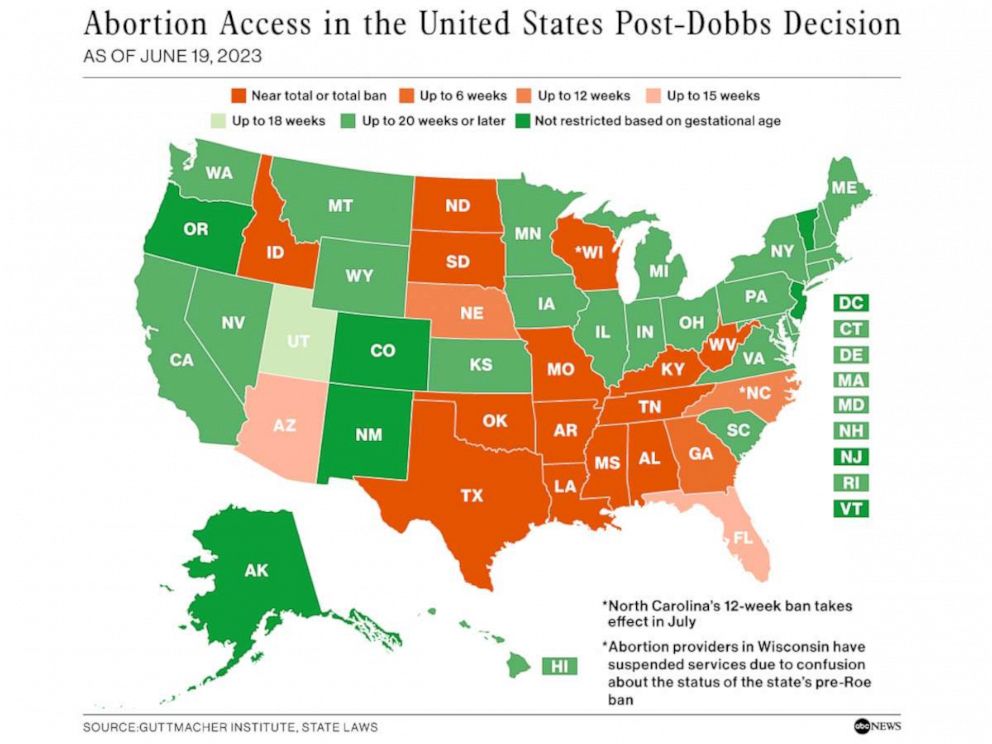
Take, for example, the case of Idaho, which on the abortion issue is the only extreme-red state (actually, dark orange in the map above) in the western part of the U.S. Idaho now has the country’s most brutal anti-abortion rules. Even before Roe v. Wade was overturned the state was experiencing shortages of medical personnel; in 2022, nine thousand health care positions went unfilled. The situation is more dire now, particularly in obstetrics and gynecology. Planned Parenthood and other similar clinics have closed all over the state. These closures affect access not only to abortion and contraception, but also to affordable mammograms and cervical cancer screening, fertility and adoption counseling, and the myriad other services that such clinics provide.
Two Idaho hospitals, citing great difficulties in recruiting skilled doctors and nurses, closed their entire labor/delivery units this past spring. According to a March 2023 press release from Bonner General, which is a major network of hospitals and clinics in Idaho, “highly respected, talented physicians are leaving… the Idaho legislature continues to introduce and pass bills that criminalize physicians for medical care nationally recognized as the standard of care.”
A recent survey of Idaho doctors working in maternal and fetal health found that of the 75 contemplating leaving the state, 73 cite Idaho’s abortion laws as a contributing factor in their decision. By the end of 2023 more than a dozen labor and delivery doctors—including five of Idaho’s nine most recognized maternal-fetal experts—will have either retired or left to practice elsewhere. Given the horrendous reputation of the Idaho state legislature for imposing restrictions on obstetric and gynecological practice, the chances of being able to replace those lost specialists are slim to none. Idaho obstetrician Amelia Huntsberger, an expert on maternal mortality, has moved to Oregon. She explained her decision by complaining that “Idaho calls itself a ‘pro-life state,’ but the Idaho Legislature doesn’t care about the death of moms.” And in May the chief doctor at one of Boise’s best hospitals told CNN that “we’re at the beginning of the collapse on an entire system of care.”
Ironically, the laws the state legislators are so proud of seem not to be reducing the numbers of abortions of Idaho’s women at all. Conservative politicians crow that there have been 1,230 fewer abortions in the state than in the year before Roe v. Wade was overturned. But the neighboring states of Washington, Oregon and Nevada respectively have reported 1,490, 1,320, and 2,580 more abortions than in the year before. Of course, not all of the excess procedures in those states are done on Idaho women. Washington clinics, for example, are serving increasing numbers of women from Alaska, Texas, and other red states as well as Idaho (in part because Governor Jay Inslee has declared Washington a “sanctuary state” whose police are barred from cooperating with out-of-state police who attempt to investigate abortion “crimes”). But in the months since Idaho passed the nation’s most extreme anti-abortion laws, the number of Idaho patients in the ten abortion clinics of eastern and central Washington—i.e., within about 150 miles of the Idaho border—has jumped by 56%. Bottom line: despite their sanctimonious blustering, the Idaho legislators have done nothing but put the health and welfare of their citizens in great danger.
Sources: Danny Westneat, “In the Washington v. Idaho abortion wars, data shows Idaho is losing,” The Seattle Times, June 28, 2023; Lauren Gallup and Rachel Sun, “Number of Idaho abortion patients traveling to Washington up 56% after Roe overturned,” Oregon Public Broadcasting, July 10, 2023; Sheryl Gay Stolberg, “As Abortion Laws Drive Obstetricians from Red States, Maternity Care Suffers,” The New York Times, September 6, 2023.
Comstockery is the world’s standing joke at the expense of the United States. Europe likes to hear of such things. It confirms the deep-seated conviction of the Old World that America is a provincial place, a second-rate country-town civilization after all.”
George Bernard Shaw, 1905
Beginning in the 1870s, the so-called moral purity campaigner Anthony Comstock (1844-1915) and his fellow zealots of the New York Society for the Suppression of Vice pressured Congress to enact a series of anti-obscenity laws. The laws called for the banning of “smutty” literature, “indecent” plays, and “articles of immoral use” such as condoms, “womb veils” (diaphragms), and pessaries (rubber devices inserted into the uterus to prevent pregnancy). The laws particularly penalized mail distribution of forbidden articles including “every article or thing designed or intended for the prevention of conception or procuring of abortion” (1876 congressional statute, amended from the initial 1873 law). Many states put some version of this federal law on their books, and this class of legislation came to be known as the Comstock Laws.
In 1883 Funk & Wagnalls published Comstock’s Traps for the Young. The book is a diatribe against what Comstock saw as rampant immorality (see below). It sold well, and was published in several editions.
*******
Selected quotes from Traps for the Young:
Satan lays the snare, and children are his victims.”
“Our youth are in danger; mentally and morally they are cursed by a literature that is a disgrace to the nineteenth century. The spirit of evil environs them.”
“But worse than any cyclone or tornado is this silent influence [ads in newspapers], this breath of poison which is breaking over our youth, destroying the brightest intellects, crushing and wounding the most lovely forms, and grinding down its victims to the lowest depths of shame and degradation.”
“The most popular plays are those in which the greatest number of brazen-faced, abandoned young women can be got together to make a public exposure of their shame… Our youth become inflamed with lust. Breathing this atmosphere, they find the pure atmosphere of home intolerable. Often they go directly from these playhouses to the brothel, or if they return home it is to dream over the obscene and cursed spectacles they have witnessed.”
“There is no force at work in the community more insidious, more constant in its demands, or more powerful and far-reaching than lust. It is the constant companion of all other crimes. It is honeycombing society. Like a frightful monster it stands peering over the sleeping child to catch its first thoughts upon awakening.”
“I repeat, lust is the boon companion of all other crimes. There is no evil so extensive, none doing more to destroy the institutions of free America. It sets aside the laws of God and morality; marriage bonds are broken, most sacred ties severed, State laws ignored, and dens of infamy plant themselves in almost every community, and then reaching out like immense cuttlefish, draw in from all sides our youth to destruction.”
*******
Comstock was delighted that his anti-obscenity crusade gave him national visibility, and he portrayed anyone who objected as “liberals and infidels.” He fumed that liberals “zealous to be known as opposed to God and religion” used quotations from Comstock’s rants to provoke laughter when they held rallies against the Comstock Laws.
Comstock frequently boasted about his triumphs in getting newspapers to stop accepting ads for abortionists and abortifacient preparations. Other sources disagreed. The vehemently anti-abortion historian Marvin Olasky lamented that enforcement of the Comstock Laws was so lax that less than two years after passage of the 1873 law newspapers such as the New York Herald were flagrantly violating it. And Comstock himself admitted that many strong state laws against disseminating contraceptives and abortifacient preparations were not being enforced. He was furious that even when violators of the Comstock Laws were brought to trial, juries and judges were loathe to convict.
Comstock claimed that his seizures of obscene items would fill many boxcars. Among his confiscations he listed 4,185 “boxes of pills, powders, etc. used by abortionists.” When one considers how ubiquitous abortion providers were in the late 19th century and how many manufacturers of contraceptive and abortifacient preparations flourished in the U.S., Comstock’s haul was actually quite meager. No doubt his boxcars were mostly filled with other items he deemed obscene, such as half-dime novels, theatrical romances, and much of classical art and literature (“some of the most obscene and foulest matters [are] the natural outgrowth of corrupt minds of past ages”).
When I taught intro to gender studies, which included a lecture on the history of reproductive rights before Roe v. Wade, I would tell students about Comstockery. They were entertained by Comstock’s ravings, as students often are by the bizarre beliefs that in earlier times were considered mainstream. It didn’t occur to me then that there were probably numerous Comstock-type laws still on the books in various states; but it turns out that that is the case. Legislators in the red states are resuscitating previously moribund Comstock-era laws to add to their arsenal of weapons to attack women’s reproductive health rights.
George Bernard Shaw would be astounded that in the 21st century in much of the country America remains “a provincial place, a second-rate…civilization.”
Sources: Constance M. Chen, “The Sex Side of Life”: Mary Ware Dennett’s Pioneering Battle for Birth Control and Sex Education (New York: The New Press, 1996); Anthony Comstock, Traps for the Young (New York: Funk & Wagnalls, 1890, 3rd ed); Marvin Olasky, The Press and Abortion, 1838-1988 (Hillsdale, NJ: Lawrence Erlbaum, 1988).
For some people, the title of this blog post might conjure up memories of the old Elvis Presley film of that name. “Blue Hawaii” featured gorgeous Hawaiian scenery, implausible shots of Elvis supposedly surfing, and pretty much everyone in the movie routinely mispronouncing the islands’ names as ha-WHY and ka-WHY rather than ha-WHY-ee and ka-WHY-ee.
For my purposes, I am more interested in the sociopolitical meaning of “blue” states as opposed to “red” states in recent U.S. history. Put simply, the blue states are those in which women’s rights, the right to health care, and humane policies are still valued and defended. These are states in which reproductive health rights are not under siege, states whose citizens have successfully resisted gerrymandering that disenfranchises Black voters, states that have not approved any anti-women legislation, such as fetal personhood measures.
Most people are not aware that Hawai`i legalized abortion in advance of the 1973 U.S. Supreme Court decision Roe v. Wade, slightly before New York and California did so. The relatively easy passage of a liberal abortion law in Hawai`i has been attributed to the multi-ethnic, multi-religious composition of the state. The relevant stakeholders, from feminist activists to politicians to physicians to ordinary citizens, appear to have viewed abortion law reform as an affirmation of shared commitment to Hawai`i’s pluralistic society as well as a way to improve women’s reproductive health options. And despite recent efforts by conservative, misogynist zealots, abortion rights are not under threat in blue Hawai`i.
Interestingly, promoters of abortion law liberalization in the early 1970s do not appear to have particularly emphasized indigenous Hawaiian attitudes toward the practice of abortion. This might have been because people living in Hawai`i circa 1970 were not yet experiencing the widespread renaissance of interest in indigenous Hawaiian language and culture that started a decade or so later. Now, however, as stated on the book jacket of the 2022 printing of June Gutmanis’ immensely influential The Secrets and Practice of Hawaiian Herbal Medicine, Hawaiian herbal medicine “is emerging as a popular alternative to traditional [i.e., modern allopathic] medical practices today.”
Originally published in 1976, this book is a classic. The late June Gutmanis was a renowned author and researcher who contributed greatly to the revival of Hawaiian culture and traditions.
Gutmanis’ book was first published in 1976 and has been continuously in print since then. At first glance, she seems an unlikely author for such a well-regarded compendium of Hawaiian herbal lore. Born in 1926 in Nebraska, she served as a pilot in World War II. She never got an academic degree but was an avid amateur historian and a founding member of the East Hawai`i Historical Society. She interviewed many kahuna (Hawaiian healers) herself and supplemented her first-person accounts with little-known archival materials.
Gutmanis explains that before European contact Hawaiian youth were expected to experiment sexually from a relatively young age. Girls and young women were taught several methods of herbal contraception, and there was no stigma attached to using them. Couples could use birth control to limit or space out their children, or even to not have children at all if that was their choice; and women who had their children too close together were scorned. To illustrate the acceptability of childlessness in old Hawai`i, Gutmanis quotes Hawaiian folklorist S. M. Kamakau, writing in 1870: “A man and a woman might live together from the time they were young and strong and full of hope until old age approached without having a child or children.” The elders of the community would help the couple prevent pregnancy.
Koa and other tannin-rich leaf tampons are among the pre-coital contraceptives mentioned by Gutmanis’ sources. Parts of the hau tree were also used, though Gutmanis laments that her sources don’t specify the parts used. She speculates that the tree’s bark, which produces a thick, mucus-like sap “may have been used as a spermicide.”
As in most indigenous (and modern) societies about which something is known of contraceptive practices, abortion was also employed for birth control. Indeed, the Hawaiian language has seven words for abortion. Abortifacient plants such as noni (Indian mulberry), hau, and `ohi`a `ai (mountain apple) could be taken orally to induce abortion. An alternative was for the woman to squat over a steam bath infused with parts of the above plants as well as several others. Surgical abortion with a sharp bamboo blade was sometimes used, but, according to Gutmanis’ sources, was more dangerous than the herbal methods.
Hot infusions of `ohi`a `ai (Mountain apple) were one of the methods traditionally used to induce abortion.Eating Noni (Indian mulberry) was traditionally believed to induce abortion.
Sources: June Gutmanis, The Secrets and Practice of Hawaiian Herbal Medicine; Honolulu: Island Heritage, 2013 (2nd edition; 1st edition 1976); Patricia G. Steinhoff and Milton Diamond, Abortion Politics: the Hawaii Experience; Honolulu: The University Press of Hawaii, 1977.
Recently, an old friend, mathematician David Rohrlich, urged his colleagues in the American Mathematical Society to refuse to hold meetings in any state that has implemented stringent anti-abortion legislation. His reasoning is simple—the laws are so vaguely written and so far-reaching in their implications that they endanger the life and health of any woman unfortunate enough to suffer a pregnancy complication while attending a professional meeting in one of the misogynist red states. Pregnant women should not be forced to choose between missing a meeting that’s professionally important to them or else risking serious illness and death if they go to the meeting.
The reaction to Rohrlich’s proposal among mathematicians has been very positive, and there’s a good chance the Math Society will announce a boycott. If other professional societies can be persuaded to do likewise, the economic effect will put pressure on the red states to stop violating women’s human rights.
The new wave of anti-abortion measures has had an unsurprising effect on women’s ability to procure an abortion. After all, the status of women’s reproductive rights in the red states was dire enough before the overturning of Roe v. Wade. What seems to have blindsided some observers, however, are the calamitous consequences of the legislation for the health and safety of any woman whose pregnancy develops complications.
The U.S. is an extremely litigious as well as highly bureaucratic society. The media are full of accounts of hospital administrators directing their medical staff to err on the side of caution when deciding what care they can give women whose pregnancies are in danger. Hospital legal teams are apparently terrified that their physicians will be charged with abortion-related criminal offenses. Obstetricians, gynecologists, and nurse-midwives are increasingly afraid to provide miscarriage treatment they would have unhesitatingly offered in previous times. Instead, medical practitioners in the anti-woman states are delaying decisions about how to treat pregnancy complications, turning away pregnant women experiencing bleeding, cramping, or elevated blood pressure, and advising the affected women to seek care in a more woman-friendly state.
In the “A Little Bit Pregnant” chapter of Sex and Herbs and Birth Control I touch on the many ways that pregnancy is a process, not an absolute. In most cultures and time periods a woman was not considered pregnant until she declared herself to be so; anything she did before that declaration to either support or discontinue her pregnancy was her own business. Even now, medical authorities view pregnancy as an unfolding process, one that begins not with sperm meeting egg, but rather with secure implantation of the fertilized zygote in the uterine wall.
In like manner, the termination of pregnancy can be a complex process. But the new laws of the red states are making the treatment of pregnancy complications hazardous, even life-threatening. As any reputable obstetric professional will tell you, the procedures to deal with a failing pregnancy are indistinguishable from those used to cause an abortion. And indeed, as journalist Kate Zernike notes, major medical societies as well as insurance providers “define abortion as any procedure that terminates a pregnancy—whether that pregnancy is wanted or unwanted, whether a woman is seeking the procedure to clean out her uterus after a miscarriage, or because of a dire fetal diagnosis, or to terminate a pregnancy she had not expected.”
But the safest methods to terminate a morbid pregnancy, while giving the patient the best chance of carrying a pregnancy to term in the future, require that treatment begins before the fetal heartbeat has ceased. Waiting for the cessation of fetal heartbeat, as the laws of several states now mandate, puts the woman at great risk of future harm.
As I mentioned above, health professionals in the anti-women states are delaying treatment or urging the affected women to travel to one of the states that puts a priority on maternal health. Clearly, this option is not equally available to everyone. The costs can be prohibitive and medical insurance often does not cover trips out-of-network. As the president of the American Medical Association noted in an article in the New York Times, the post-Roe situation is causing “chaos.” As Zernike succinctly puts it: “Women are being denied abortions for miscarriages and to end pregnancies that have little or no chance of survival or left to become sicker before they can have an abortion deemed to be lifesaving.”
The risks of pregnancy complications in the U.S. are significantly higher than in other industrialized countries. Reasons include a higher percentage of first pregnancies among older women, a large percentage of expectant women with high blood pressure, diabetes, and obesity, COVID-19 sequelae, and expensive or otherwise inaccessible pre-natal care options. Cases of preeclampsia, stillbirth, ectopic pregnancy, and other morbid conditions are high and increasing. Women experiencing these conditions often need abortion care sooner rather than later. These issues are not going away, despite anti-women politicians’ attempts to sweep the consequences of their vicious policies under the rug.
Among sources consulted: Kate Zernike, “After Roe, a Debate About What the Word ‘Abortion’ Means,” New York Times, 10/18/2022; Ariana Eunjung Cha, “Pregnancy complications spiked during the pandemic,” Washington Post, 10/8/2022. The New York Times also has a series of video interviews with health professionals and others that can be accessed online.
Law students demonstrate at the U.S. Supreme Court after learning of the leaked anti-abortion decision.
For many months, ever since far-right jurists became the majority on the U.S. Supreme Court, it has been expected that the Court would soon either drastically curtail or entirely overturn the historic 1973 decision Roe v. Wade that recognized women’s abortion rights. On May 2 the most dire predictions were confirmed. A 90-page draft copy of Justice Samuel Alito’s majority ruling completely overturning Roe v. Wade was leaked to the press. That the draft document made its way into the media prematurely is an unprecedented scandal in and of itself. But the contents of the document are far more shocking than the circumstances in which it became known. In the most dramatic rejection of women’s rights in recent U.S. history, the Court majority will reverse Roe v. Wade and the past fifty years of Federal court decisions reaffirming reproductive rights. The U.S. will join Poland, Nicaragua and El Salvador as one of only four countries that have rolled back access to abortion during the last three decades. Meanwhile, since 1994 fully fifty-nine countries have expanded the conditions under which abortion is legal.
This blog has quite a number of readers from outside of the U.S., so it bears repeating that the Supreme Court decision will not criminalize abortion in the entire U.S. The woman-friendly “blue” states, including most states in the northeast and coastal west of the country, will keep abortion legal and accessible. But their resources are likely to be strained by having to accommodate women fleeing the draconian restrictions in the misogynist “red” states. The hospital system of my state of Washington, for example, has been greatly taxed by an influx of seriously ill Covid-19 patients who contracted the virus in the neighboring state of Idaho, where the anti-mask and anti-vaccine movement is strong, and is generally supported by Republican political authorities. Now, with the Supreme Court opening the door to anti-abortion legislation in Republican-controlled states, clinics in Washington are anticipating an increase of Idaho women fleeing to our state to escape Idaho’s abortion ban.
As many commentators have noted, the woman-friendly states generally protect access to a full range of reproductive health options. In addition to abortion, often with state-assured financing for poor women, such states also provide access to low cost or free contraceptives, prenatal and postnatal care, and other services for infants and children. Meanwhile, the misogynist states such as, for example, the anti-abortion stronghold of Mississippi (whose recent legislation restricting abortion Alito cites favorably), have some of the worst statistics in the country on women’s and children’s health and welfare.
In the ruling Justice Alito blames his predecessors’ decision in Roe v. Wade for inflaming divisiveness in the U.S. over the abortion issue. The truth of the matter is that it is the extremist anti-abortion decision by Alito and his confederates that will lead to disputes and conflicts among the states. By throwing decisions on abortion legality exclusively back into the hands of the individual states, the U.S. Supreme Court is exacerbating the already immense divide between the roughly half of the country whose policies and laws provide for reproductive health rights, and those deeply misogynist regions with blatant disregard for the health and welfare of women.
There is widespread agreement among historians that the worst decision ever made by the U.S. Supreme Court was the Dred Scott decision of 1857, which held that a Black person could not have the rights and protections of a citizen, even in a free state where slavery was not permitted, and, moreover, could be taken to a slave state and re-enslaved. According to the Wikipedia article on the Dred Scott decision, “Although Taney and several other justices hoped the decision would permanently settle the slavery controversy, which was increasingly dividing the American public, the decision’s effect was the complete opposite. Taney’s majority opinion suited the slaveholding states, but was intensely decried in all the other states. The decision inflamed the national debate over slavery and deepened the divide that led ultimately to the Civil War.” Apparently Alito and his fellow rightists on the Court would rather disregard the lessons of history.
According to the Guttmacher Institute, the year 2021 saw the passing of the largest quantity of anti-abortion legislation since 1973, when a woman’s Constitutional right to have an abortion was established in the U.S. And the U.S. Supreme Court still seems on track to either drastically weaken or overturn Roe v. Wade this summer. Amid all the depressing news, however, there are some bright spots. Most of the positive developments are outside of the U.S.—the vocal and successful women’s reproductive rights campaigns in various countries of Latin America, for example. But a few recent actions in the U.S., including several by companies in the state of Texas, have pushed back against the vicious misogyny of many state legislators and their supporters.
Citigroup, a major financial enterprise with over 8,000 employees in Texas, has announced that it will pay travel costs for any of them who are affected by SB-8. This is the Texas law that not only bans abortion after six weeks, but also threatens lawsuits against anyone involved in assisting someone to circumvent the law (for example, by facilitating travel of a Texas resident to a more woman-friendly state).
The transportation companies Lyft and Uber have also announced policies in defiance of SB-8. They have offered to pay expenses for any of their Texas-based drivers who might get sued for taking a woman to an abortion clinic.
Yelp, the online search and review company, has said that their over 200 employees in Texas will be reimbursed for expenses if they need to travel out of state for abortion care. Moreover, representatives of Yelp have stated that the reproductive health guarantees offered to their Texas workforce will be extended to their employees in any state who might face “current or future action that restricts access to covered reproductive health care.” Employees will be able to submit their requests for reimbursement of abortion-related medical expenses directly to Yelp’s health insurance provider, so neither fellow Yelp workers nor officious misogynists trying to enforce SB-8 or similar legislation will be able to track the persons involved. This latest action builds upon several years of Yelp’s efforts in support of abortion rights. The company does not allow anti-abortion entities of the “crisis pregnancy center” type to portray themselves neutrally or masquerade as abortion clinics. And in the months leading up to the passage of SB-8 Yelp offered to double-match employees’ donations to reproductive health rights organizations opposing the legislation.
Yelp and Citigroup will support the expenses of employees in Texas who need to travel out of the state for abortion or other reproductive health needs; Uber and Lyft will cover the expenses of any driver who is sued for transporting a woman to get an abortion.
Meanwhile, back in the state of Maryland legislators are the latest to take a stand in defense of reproductive health rights. A bill scheduled to take effect July 1 of this year allows nurse practitioners, nurse midwives, and trained physicians’ assistants to perform abortions, requires insurance providers to cover abortion costs, and apportions $3.5 million per year for abortion training. Maryland’s Republican governor Larry Hogan vetoed the bill, but under the leadership of the Speaker of Maryland’s House of Delegates, Democrat Adrienne A. Jones, the House overrode the veto by a vote of 90 to 46; and the state Senate concurred with a 29 to 15 override. Maryland joins California, Colorado, Connecticut, Hawaii, Illinois, Maine, Massachusetts, Montana, New Hampshire, Oregon, Vermont, Virginia, Washington and West Virginia in permitting abortion to be performed by medical professionals other than physicians, and it is one of sixteen states that provide at least some state funds for abortions.
Sources for this piece include the Guttmacher Institute website and April 10 and April 12 articles in the New York Times.
Adrienne A. Jones, Speaker of the Maryland House of Delegates
Washington University in St. Louis, Missouri has a world-renowned medical school and affiliated teaching hospital. In the early 20th century, one of its most distinguished professors was the obstetrician and gynecologist Frederick J. Taussig.
Prominent American gynecologist Dr. Frederick J. Taussig (1872-1943)
Taussig wrote extensively on abortion, and his work was frequently cited by other experts; I read both of his major treatises when I was writing Sex and Herbs and Birth Control and purchased my own copies on E-Bay. Taussig was a careful observer, and unlike most physicians of his era he was willing to acknowledge the superior skill of midwives in providing safe abortions. Taussig also believed that more married men should take responsibility for contraception by having a vasectomy, since it was an outpatient procedure and “perfectly harmless.” He lamented that “it is as yet difficult to persuade many men to undergo this slight sacrifice for the sake of their wives.”
In 1910, when Taussig published his first major treatise, like most of his professional colleagues he was vehemently opposed to the legalization of abortion. But over the course of his career (and under the influence of his wife Florence Gottschalk, who was a prominent Suffragette) Taussig began to advocate wide-ranging reform of the law codes. He put his support for legalization firmly in a feminist context. In his 1936 volume on the subject, Dr. Taussig noted: “With the spread of the Woman’s Suffrage Movement throughout the world and the newer independence of women, the revolt of womankind against the age-long domination of man has finally materialized. There can be no question that more consideration must be given to the right of women to control their own bodies…. Thus far all laws and social regulations on abortion have been man-made, and women, who are the chief sufferers, have had no chance to express their views in any referendum.”
Dr. Taussig’s 1936 book was extremely influential among physicians and others with an interest in maternal health. His comprehensive scientific treatment of both spontaneous and induced abortion along with his sensitivity to social context made his work the standard reference on the subject for decades, as both supporters and opponents of abortion law reform have acknowledged.
The most important book on abortion in the pre-War period (published in 1936)
Dr. Taussig insisted on viewing abortion as a necessary component of gynecological training, and under his tutelage medical students gained the expertise they needed to safely perform abortions and tend to complications of pregnancy.
It is a terrible irony that the Washington University School of Medicine, after so many years of being a national leader in women’s reproductive health, is now increasingly under attack by the Missouri State Legislature for its efforts to provide the next generation of physicians with the training they need.
The American College of Obstetricians and Gynecologists (ACOG) recommends standardized education on abortion in all residency programs (in which U.S. physicians-in-training work in a teaching hospital for three years to gain practical experience in their specialty after they finish medical school). But it is a sad fact that fully half of U.S. medical schools do not offer training in abortion care, or at most offer one lecture on abortion and contraception combined. In order to keep their accreditation, hospitals with residency programs in obstetrics and gynecology are required to either provide abortion training themselves or allow their residents to go out of state to obtain it. As it stands now, Washington University students need to go to Illinois for their abortion training. Yet state legislators want to tax the university’s endowment on the grounds that, as Republican Mike Moon put it: “Washington University is a premier institution which trains students to perform abortions… These students are then hired to murder developing human babies across our nation. They won’t stop on their own. This [bill] will place a financial hardship on their ability to train these students.”
States such as Missouri, Texas and Idaho are not only greatly restricting the conditions under which abortion can be legally obtained. They are also threatening to prosecute anyone who teaches abortion techniques, seeks an abortion outside of the state, or performs an abortion on a state citizen regardless of where the procedure is done. Whether or not such laws will withstand court challenges, and whether or not the laws could be enforced in practice, they have an intimidating effect on medical professionals as well as on women seeking a full range of reproductive health options.
The competition to obtain a place in a residency program in a woman-friendly state in which training in abortion is not under attack has become more severe. As medical reporter Sarah Varney put it: “Increasingly, aspiring obstetricians and gynecologists who want training in abortion procedures are seeking out teaching hospitals and universities that champion that training as a vital skill in women’s health care, creating a crush of qualified applicants for prized spots in Seattle, San Francisco, and New York…”
The medical school of the University of Washington (UW) in Seattle is offering Zoom classes on contraception and abortion to medical students in Idaho, one of the many states that are drastically restricting abortion and access to abortion training. As of two years ago UW stopped reserving a few spots in their program for residents choosing not to learn abortion care. “If we live in a state where abortion care is legal, we need to recruit medical students into our program that want to provide abortion care,” said Dr. Alyssa Stephenson-Famy, an associate professor of maternal-fetal medicine in the department. “We should not waste our spots on people not willing to provide abortion.”
It bears stressing that state legislators are delusional if they think that obstetricians and gynecologists can be properly trained without understanding abortion care techniques. ACOG requires abortion training for medical residents because adequate care of pregnant women is impossible without knowledge of the basic procedures. Obstetricians must be capable of expertly cleaning out a woman’s uterus in the event of a miscarriage or if fetal heartbeat ceases. As Dr. Eve Espey, a professor of obstetrics and gynecology at the University of New Mexico, has observed: “Any obstetrician who says there is never need for abortion care is not telling the truth about obstetrics.”
Sources: Sarah Varney, “Fewer medical students trained for abortion procedures,” NBC News online, March 22, 2022; Frederick J. Taussig, The Prevention and Treatment of Abortion (1910) and Abortion: Spontaneous and Induced (1936).
Latin American reproductive health rights activists have logged another victory. Last week the Constitutional Court of Colombia (the highest court in the country) voted five to four to decriminalize abortion in the first twenty-four weeks of pregnancy. Colombia thus joins Mexico and Argentina in decriminalization, which means that three of the four most populous countries of the region have taken a major step toward making abortion legal and accessible. (Brazil’s vocal feminist movement is pushing for legalization, but so far has had no success.)
Colombian reproductive health rights activists are quick to point out that their victory owes a lot to their relationships with activists in other parts of Latin America. The Colombians consulted with movement lawyers from Mexico, adopted street theatre performances originating in Chile, and wear the distinctive green kerchiefs first used by women activists in Argentina.
Latin American feminists know that the constant sharing of strategies and tactics across the region has made all of their movements stronger and more vibrant. They contrast their recent successes with the string of TRAP laws in many U.S. states and the ominous probability that the U.S. Supreme Court will reverse Roe v. Wade this summer. Catalina Martínez Coral, a lawyer and member of Causa Justa, the coalition of abortion rights groups that brought the relevant case to the Colombian Constitutional Court, noted that the waves of feminist activism are “now an inspiration going south to north… We are going to inspire people in the United States to defend the rights set out in Roe v. Wade.” Serra Sipel, the chief global advocacy officer at Fòs Feminista, an international alliance of reproductive rights groups, agrees, saying “We in the U.S. can really learn a lot” from Latin American feminist organizations.
Some of the roots of Colombia’s reproductive rights movement can be traced back to a visit to the U.S. by the eminent Colombian obstetrician/gynecologist Dr. Jorge Villareal Mejía. Dr. Villareal toured some of the first legal abortion clinics that opened after the Roe v. Wade decision and decided to find a way to offer similar services in his homeland. In 1977, he opened the first of his Oriéntame clinics in Bogotá. The clinics offered a full range of reproductive health services, including abortion. They charged on a sliding scale, and their promotional materials delicately urged their more affluent clients to contribute to the costs of procedures for poorer women.
Dr. Jorge Villareal Mejía (1927-2001)
I have known about Oriéntame since the early 1990s. Before full legalization of abortion in Colombia I referred to it by a pseudonym in my writing, in particular in my book Sex and Herbs and Birth Control.
Under Dr. Villareal’s direction the clinics pursued a remarkable two-pronged strategy. On the one hand, Oriéntame skirted the question of illegality of abortion by labeling its services as “walk-in patient treatment of incomplete abortion.” As a medical director of the organization once explained to me, a sympathetic Jesuit priest reconciled his support for Oriéntame with the Catholic view of abortion as a sin by reasoning that once a woman decided in her mind to have an abortion, she had begun the process. Oriéntame personnel were merely aiding her to complete her abortion safely. And indeed, in the forty-five years of their existence the clinics have performed close to a million abortions with a vanishingly small number of serious complications.
The second aspect of Dr. Villareal’s vision involved a brilliant outreach program. To quote from Sex and Herbs and Birth Control (in which I referred to Oriéntame as CRH, or Centers for Reproductive Health): “CRH offers scholarships to midwives and doctors from other areas of Central and South America who might want to set up similar clinics. They have trained over 600 physicians, nurses, physicians’ assistants, and traditional as well as licensed midwives in vacuum aspiration abortion techniques; their students perform abortions in clinics in Bolivia, Colombia, Ecuador, Guatemala, Mexico, Paraguay, Peru, Uruguay, Venezuela, and elsewhere…. In Peru I met a director of the country’s society of women obstetricians who had attended the program and was an enthusiastic advocate of the idea; I’ve run into CRH graduates in Nicaragua and Chile as well.”
Oriéntame personnel have not only trained numerous reproductive health specialists from all over the region in the latest abortion techniques. They have also shared their expertise in how to make use of the legal exceptions in various law codes to increase women’s options. As Giselle Carino, an Argentinian activist in Fòs Feminista, noted: “Without a doubt, we learned from the Colombians.”
Although for large portions of its history Oriéntame managed to steer clear of police harassment, a spate of incidents in 1994 encouraged Dr. Villareal’s daughter Cristina, who was taking over directorship of the organization from her father, to reach out to feminist groups in order to unite with medical practitioners to try to change Colombia’s laws. Cristina Villareal joined with others to form the coalition La Mesa por la Vida y la Salud de las Mujeres. In 2006 the group’s efforts caused a broadening of legal exceptions in which abortion was permitted in Colombia, and full decriminalization through twenty-four weeks was achieved in late February of this year.
Oriéntame and its international training program continue to offer reproductive health services in Colombia, train physicians, midwives, and healers, and advise affiliates on the best ways to navigate legal pitfalls. But, as feminist activists in Latin America know and their counterparts in the U.S. are finding out, it does not pay to be too complacent. As Cristina Villareal warns, “This is a battle that is never completely won… You can’t let your guard down.”
Sources for direct quotes are February 21 and 23, 2022 New York Times articles by Julie Turkewitz. Additional information can be found at https://orientame.org.co (Spanish) and https://orientame.org.co/en (English).
January 23, 2022 marked the forty-ninth anniversary of the landmark U.S. Supreme Court decision Roe v. Wade. Unfortunately, given the current right-wing composition of the Court, Roe v. Wade is unlikely to make it to the fiftieth anniversary. The Court is expected to uphold a Mississippi law prohibiting abortion after fifteen weeks from a woman’s last menstrual period, which is at approximately thirteen weeks of fetal gestation. Mississippi’s governor has repeatedly boasted that the state will continue its efforts to make Mississippi “abortion-free,” and he and his supporters have drafted a number of anti-abortion laws that will go into effect as soon as Roe v. Wade is overturned. Conspicuously absent from any of this bluster is any attempt to improve the lot of pregnant women, including those who wish to bring their pregnancies to term. Mississippi does a horrendous job of protecting pregnant women, mothers, and newborns.
Mississippi is not the only state whose legislators are eagerly awaiting the demise of Roe v. Wade. It is also not the only state whose politicians style themselves as “protectors” of pregnant women and their fetuses. As in other states in this category, the sanctimonious pronouncements hide a sordid reality of neglect and unconcern for those the grandstanders claim to value. Mississippi is woefully inadequate in providing prenatal care to its large population of uninsured pregnant women, ranks worst in the nation in health care access and quality, and has the second-highest rate of teen pregnancies in the U.S. (after Arkansas). It also has high rates of infant mortality, premature births, and low-birth-weight infants.
As it turns out, the same coercive circumstances that make abortion access difficult or impossible in many parts of the U.S. also contribute to bad outcomes for pregnant women and newborns. It’s well known that the U.S. has the highest rates of maternal and infant mortality in the industrialized world. The rates vary widely by region of the country and economic circumstances, with anti-women states like Mississippi leading the way and with the greatest negative impacts on women of color and the poor. Despite pious platitudes about protecting women and “the unborn,” these states stand out for their callous treatment of women seeking to carry their pregnancies to term.
Recently, I reviewed a book by Louise Marie Roth titled The Business of Birth: Malpractice and Maternity Care in the United States (New York University Press, 2021). I confess, I wasn’t super-enthused at first. The subtitle seemed to suggest a rather narrow focus on the intricacies of U.S. tort law and the details of malpractice suits stemming from unfortunate outcomes for pregnant women and newborns. However, in reality the book has a much broader scope. The author paints a fascinating, albeit often distressing, picture of the complex interactions of medical practitioners, hospital administrators, insurance providers, malpractice attorneys, and state legislators. Often the result is a toxic mix of circumstances leading to huge numbers of unnecessary Caesarian sections and chemically induced deliveries, coercion of pregnant women (especially poor, rural, and minority women), outrageously expensive pregnancy care, and, as noted above, the highest rates of maternal and infant mortality in the developed world. Roth supplements her analyses of changes in law codes and standards of care with interviews with obstetricians, nurse-midwives, lawyers, and insurance adjusters. The upshot is that less affluent and less educated women can be pressured into episiotomies and repeated Caesarian sections, rendered virtually immobile during labor by the exigencies of constant electronic fetal monitoring, and have their deliveries artificially induced on a Friday so obstetrical staff don’t need to come in on the weekend (resulting in the weekend birth decline notable in many U.S. hospitals).
Roth describes the misleading and often false information medical personnel cite to compel women to consent to procedures that in many cases are unnecessary, expensive, and possibly harmful. Repeated Caesarian sections, for example, present increasing risks of future pregnancies ending in miscarriage or stillbirth, yet hospital administrators urge or even force them on women ostensibly because of overblown fears of malpractice suits. But nervousness about legal liability is only part of the story. In the period 1995 to 2015 the odds of a Black woman with low risk of delivery complications being given a first-birth C-section were 35% higher than for non-Hispanic white women. The odds of being coerced into repeated C-sections were also higher for Black women.
There are obvious parallels to the plethora of misinformation pushed on women seeking abortion in many states. In fact, Roth makes it abundantly clear that the same forces that constrain women’s access to abortion work to prevent many pregnant women’s access to the best care for themselves and their newborns.
Reproductive health regime
Fetus-centered
Woman-centered
Mississippi
Oregon
Infant mortality (per 1000 live births)
11.46
5.99
Maternal mortality (per 100,000 live births)
20.8
12.8
Roth distinguishes between fetus-centered and woman-centered reproductive health regimes and persuasively argues that pregnant women and their offspring are better served in states that protect abortion rights “and prioritize women’s rights over fetal life” (p. 10). She gives numerous examples of both types of reproductive health regimes. Particularly striking is her comparison of Oregon and Mississippi. Oregon has no TRAP laws, requires comprehensive health insurance to cover prescription contraceptives and abortion, permits nurse practitioners to provide both medical and surgical abortions, and covers abortion services for the poor with state funds. The state, emphatically a woman-centered reproductive health regime, has below-average rates of teen pregnancy and infant mortality, good state-supported prenatal care, and above-average maternity care outcomes. By contrast Mississippi, the epitome of a fetus-centered reproductive health regime, has a large number of TRAP laws, long mandatory waiting periods, and extreme anti-abortion measures that are set to become law as soon as Roe v. Wade is overturned (which will probably happen this summer). And, Roth would argue, not coincidentally, Mississippi has some of the worst maternal and infant mortality statistics in the country.